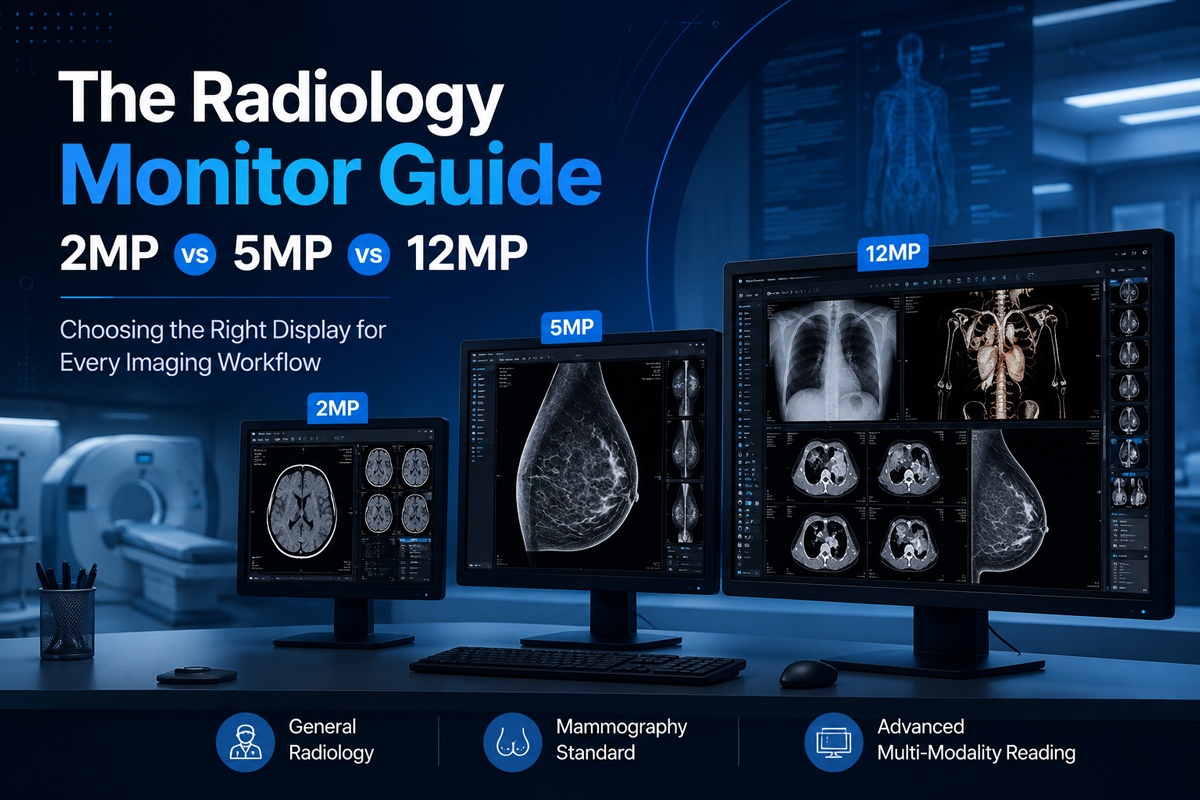
Choose a 2MP monitor for general radiology and multi-modality reading where space and budget matter. Choose 5MP for mammography and other detail-critical exams that demand fine grayscale rendering. Choose 12MP only when you consolidate multiple high-resolution images on a single screen and need every pixel auditable to regulatory standards.
A monitor that displays an image is not the same as a monitor that protects a diagnosis. Buying the wrong resolution wastes capital, slows reading throughput, and—worse—risks missing the subtle findings that define accurate interpretation. A 2MP display in a mammography suite fails to resolve micro-calcifications. A 12MP display in a general reading room burns budget on pixels no one uses.
This guide breaks down the three dominant resolution tiers in diagnostic radiology—2MP, 5MP, and 12MP—and the technical factors that determine whether a display earns its place in a clinical workflow. You will learn which modalities each tier serves, what brightness and calibration thresholds matter, and how ergonomics and compliance shape the real cost of ownership.
By the end, you will be able to match resolution to clinical need instead of marketing claims. The goal is a defensible purchase decision—one that survives an audit and serves the radiologist reading at 2 a.m.
Why radiology monitor resolution determines diagnostic accuracy
A consumer monitor and a diagnostic display share almost nothing beyond a backlight. The gap between them decides whether a faint lesion appears or vanishes.
Diagnostic Monitors exist to render every clinically relevant pixel at calibrated, verifiable luminance—consumer monitors do neither. Medical images carry far more grayscale information than standard screens can reproduce. A diagnostic display renders up to 1,024 distinct shades of gray, calibrated to the DICOM Grayscale Standard Display Function (GSDF), so that the same pixel value looks identical across every workstation in the department. Consumer monitors apply uncontrolled gamma curves that distort contrast. The result on a consumer screen: subtle density differences signaling pathology disappear into a uniform gray.
Resolution is the first variable in this chain, not the only one. It determines how much image data the radiologist sees without panning or zooming. Pick it wrong, and you either lose detail or pay for detail you cannot use.
Understanding monitor resolution: what 2MP, 5MP, and 12MP actually mean
The “MP” rating counts total pixels, not image quality. Confusing the two leads to overspending and underperforming.
Megapixel ratings describe how much image area a display resolves at once—not how accurately it renders contrast or grayscale. A 2MP monitor packs roughly 2 million pixels (typically 1200 × 1600). A 5MP monitor holds about 5 million (2048 × 2560). A 12MP monitor reaches roughly 12 million (4200 × 2800 or similar), often replacing two separate displays with one wide panel. More pixels mean more anatomical coverage and finer spatial detail before zoom.
But pixel count alone proves nothing about diagnostic fitness. A high-megapixel panel with poor luminance uniformity or an uncalibrated grayscale curve fails where it matters. Resolution sets the ceiling for detail. Calibration and luminance decide whether you reach it.
2MP monitors: the workhorse for general radiology and multi-modality reading
Many buyers assume more pixels always serve the patient better. For general radiology, that assumption wastes money and desk space.
A 2MP display meets the diagnostic requirements for CT, MRI, ultrasound, and most multi-modality reading at the lowest cost per workstation. These exams generate images whose native matrix sizes the 2MP resolution renders without loss. Radiologists reading cross-sectional studies scroll through stacks rather than scrutinizing a single high-density frame, so the 2MP format matches the workflow. The lower price also lets departments equip more workstations within a fixed budget.
The 2MP tier breaks down in one place: high-detail projection imaging. Digital mammography and chest radiography demand finer spatial resolution than 2MP provides.
| Tier | Pros | Watch-outs | Best for |
| 2MP | Lowest cost per station; fits CT/MRI/US native matrices; compact footprint | Under-resolves mammography and detailed chest X-ray | CT, MRI, ultrasound, multi-modality reading rooms |
5MP monitors: the standard for mammography and detail-critical imaging
Skimping on resolution in breast imaging is a clinical and legal exposure. Micro-calcifications measure fractions of a millimeter, and a screen that blurs them blurs the diagnosis.
A 5MP display is the recognized standard for digital mammography because it resolves the micro-calcifications and fine tissue boundaries that 2MP misses. Mammographic images carry detail at the limit of human visual acuity. The 5MP resolution renders these images closer to full native size, reducing the panning and zooming that fatigue the reader and slow throughput. Many regulatory and accreditation frameworks for breast imaging specify 5MP-class displays for primary interpretation.
The 5MP tier also serves digital radiography, tomosynthesis slices, and any modality where fine projection detail drives the read. It costs more than 2MP and demands stricter calibration discipline, but for these modalities the cost is non-negotiable.
| Tier | Pros | Watch-outs | Best for |
| 5MP | Resolves micro-calcifications; meets mammography accreditation specs; reduces pan/zoom | Higher cost; stricter calibration cadence required | Digital mammography, DR, tomosynthesis, detail-critical reads |
12MP monitors: when consolidating high-resolution images is non-negotiable
A wall of separate monitors creates bezels, color mismatch, and inconsistent calibration across panels. For some workflows, that fragmentation costs reading speed and consistency.
A 12MP display consolidates the area of two 5MP monitors into one seamless, uniformly calibrated panel—eliminating bezel gaps and cross-display luminance drift. Radiologists comparing prior and current mammograms, or viewing tomosynthesis alongside synthesized 2D images, gain an unbroken field with a single calibration target. One panel means one GSDF curve, one luminance baseline, and one calibration audit instead of two that can diverge. The widescreen format also supports flexible hanging protocols that adapt to study type.
The 12MP tier earns its premium only in high-volume, comparison-heavy workflows. For a general reading room, the pixels go unused, and the budget goes wasted. Buy 12MP when the workflow demands consolidation—not because the number is largest.
| Tier | Pros | Watch-outs | Best for |
| 12MP | Replaces two displays with one calibration target; no bezel gap; flexible hanging protocols | Highest cost; over-specified for routine reading | High-volume breast imaging, comparison reading, tomosynthesis |
Brightness, contrast, and calibration: the specifications that outrank resolution
Buyers fixate on megapixels and ignore the parameters that actually govern whether a finding appears. A high-resolution monitor with drifting luminance fails an audit and misses lesions.
Calibrated, sustained luminance and a verified GSDF curve protect diagnostic accuracy more reliably than raw pixel count. Diagnostic displays target a calibrated luminance—commonly 500 cd/m² or higher for mammography—maintained constantly through a built-in backlight sensor and stabilization circuit. Without that stabilization, brightness decays as the backlight ages, and contrast for subtle findings degrades with it. Peak nits at installation mean nothing if luminance drifts six months later.
Calibration is not a one-time event. A “DICOM-calibrated” label at purchase guarantees nothing about performance a year on.
Conformance to DICOM GSDF, verified on a recurring schedule, is what keeps interpretations consistent across workstations and over time. A front-mounted luminance sensor measures output and corrects the grayscale curve automatically, keeping every panel on the same standard. Quality-assurance software logs each calibration, producing the audit trail that accreditation bodies require. Skip the recurring check and grayscale drifts silently—two radiologists reading the same image on two stations reach different conclusions.
Luminance uniformity matters as much as peak brightness. Subtle findings fail first at the panel edges, where uneven backlighting masks low-contrast detail. Uniformity-compensation circuitry corrects brightness variation across the panel so a micro-calcification reads the same in the corner as in the center.
Ergonomics and workflow: protecting reading accuracy across a long shift
A display that strains the eyes degrades the diagnosis by the end of a shift, regardless of its specifications. Fatigue is a clinical variable, not a comfort issue.
Ambient light control and reduced eye strain directly preserve diagnostic accuracy over a full reading day. A reading room is not a static darkroom; ambient light shifts as people move and overhead lighting changes, washing out screen contrast. An Ambient Light Compensation sensor faces the room, measures incident light, and adjusts the display to hold contrast steady. Without it, the radiologist squints against glare, and low-contrast findings drop below the threshold of perception.
Workflow friction costs accuracy, too. A radiologist who navigates clumsy menus or manually adjusts settings for every study loses focus and time. Integrated presence sensors that dim the display when the reader steps away extend backlight life and hold calibration. Mounting flexibility—height, tilt, and rotation—lets each reader set an ergonomic position that sustains attention through a long list. Small interface efficiencies compound across hundreds of studies into measurable accuracy and throughput.
Future trends in radiology displays
Static specifications describe today’s monitor, not the demands arriving with AI-assisted reading and higher-bit-depth imaging. Buying without that horizon shortens the useful life of the purchase.
Displays are evolving to render higher bit depth, integrate AI overlays, and self-monitor calibration in real time. Emerging panels push beyond 8-bit grayscale toward 10- and 11-bit rendering, exposing finer density gradations as detectors and reconstruction algorithms improve. AI-assisted detection tools increasingly draw findings directly onto the diagnostic display, so the panel must render both the source image and the algorithmic overlay at full fidelity. Real-time calibration monitoring—where the display continuously verifies its own GSDF conformance and flags drift instantly—reduces the manual QA burden and tightens the audit trail.
Plan for these capabilities at purchase. A display chosen only for today’s matrix sizes becomes the limiting factor when the imaging chain advances.
Making the right resolution choice for your practice
Resolution is the starting point of a diagnostic display decision, not the whole of it. Match the megapixel tier to the modality first: 2MP for CT, MRI, and ultrasound; 5MP for mammography and detail-critical projection imaging; 12MP for high-volume comparison reading that demands consolidation. Then verify the factors that resolution alone cannot deliver—calibrated and sustained luminance, recurring GSDF conformance, uniformity compensation, and ambient light control.
The defensible purchase serves three masters at once: the radiologist who needs to see the finding, the workflow that needs throughput, and the auditor who needs proof of consistency. A monitor that satisfies all three protects the diagnosis and the department’s compliance record together.
Before you sign a purchase order, map every reading modality in your practice to a resolution tier, then confirm each candidate displays its luminance stabilization and calibration QA. Specify the right pixels, demand verifiable calibration, and the display will serve the diagnosis for years.
Frequently asked questions
What resolution monitor is required for digital mammography?
Digital mammography requires a 5MP-class display for primary interpretation. The 5MP resolution resolves micro-calcifications and fine tissue boundaries that lower-resolution panels blur. Many accreditation frameworks specify 5MP-class displays for primary breast imaging reads, paired with high calibrated luminance—often 500 cd/m² or above.
Is a 2MP monitor good enough for diagnostic radiology?
Yes—for the right modalities. A 2MP display meets the diagnostic requirements for CT, MRI, ultrasound, and general multi-modality reading at the lowest cost per workstation. It is not sufficient for digital mammography or detailed chest radiography, which demand the finer spatial resolution of a 5MP display.
When is a 12MP monitor worth the cost over two 5MP monitors?
Choose a 12MP monitor when your workflow requires consolidating high-resolution images on one panel—high-volume breast imaging, prior-versus-current comparison, or tomosynthesis review. A single 12MP panel removes bezel gaps and uses one calibration target instead of two that can drift apart. For routine reading, two 5MP displays or a single lower tier serve better at a lower cost.
Why does monitor calibration matter more than resolution?
Calibration governs whether the displayed image is accurate; resolution only governs how much of it you see. A monitor calibrated to the DICOM GSDF renders grayscale consistently across workstations and over time. Without recurring calibration, luminance and grayscale drift, producing inconsistent interpretations and failed audits—regardless of pixel count.
How often should diagnostic monitors be calibrated?
Diagnostic monitors require recurring calibration verified on a defined schedule, not a single calibration at installation. Built-in luminance sensors correct the grayscale curve automatically, while QA software logs each check to produce the audit trail accreditation bodies require. The exact cadence follows your accreditation body’s requirements and your facility’s QA protocol.
What luminance level do diagnostic radiology monitors need?
Diagnostic displays require high, calibrated luminance maintained constantly—commonly 500 cd/m² or higher for mammography. A backlight stabilization circuit holds that level steady as the backlight ages. Peak brightness at installation is irrelevant if the display cannot sustain calibrated luminance over its service life.